SpacedX
-
Posts
8,134 -
Joined
-
Last visited
-
Days Won
5
Everything posted by SpacedX
-
No, I really am not. I am wholeheartedly in agreement with you there and that wasn't what I was disputing.
-
But your argument is predicated upon the false premise that longer working hours are beneficial to the state economy. Studies have shown productivity per hour declines after employees work more than 50 hours a week and the drop off is even more pronounced after 60 hours. That there is an inverse relationship between productivity and longer working hours is now consensual. I think that it is far more likely that in the near future the state retirement age will be raised to 70 - possibly for those born on or after April 1980.
-
Obviously, disregarding some of the outright abject stupidity that has been posted on this forum, it's hard to recall a recent time in which I've so vehemently disagreed with an opinion from such and ordinarily rational member. Taking Japan as an example, who have long faced international condemnation for their excessive working hours and levels of presenteeism leading to work related stress and related health and well being issues, they are actively working to reduce working hours, with initiatives like the 'Work Style Reform' campaign. This aims to limit overtime, engender flexible work arrangements with the objective of fostering a more favourable work-life balance. The voting public simply will not accept a reversion to a longer working week and the majority of employers will oppose it. We are moving in the opposite direction. Microsoft Japan and a host of other companies, including Panasonic and Unilever, experimented with a four-day working week. Microsoft Japan's experiment in 2019 reported a productivity increase by 40%. Other companies, like Bolt and Kickstarter, who have also explored the idea still offer it several years after a successful pilot scheme.
-
 Well there was that outrageous pass against Fleetwood Town in the FA Cup, and the assist for Mahrez against Watford. So not strictly true.
Well there was that outrageous pass against Fleetwood Town in the FA Cup, and the assist for Mahrez against Watford. So not strictly true. -
People that cause unnecessary queuing at filling stations because they either lack the confidence to use the opposite side to their fuel tank filling or are completely unaware of the hose reach on fuel pumps.
-
-
Fallout IV
-
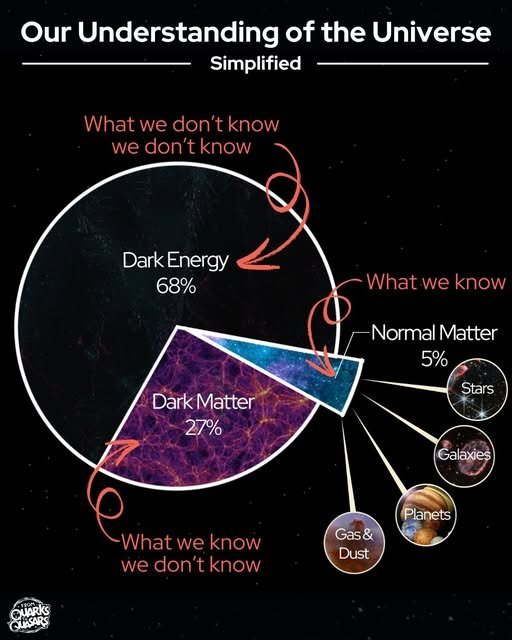
Meanwhile, on a different subject, spectroscopic analysis is not definitively conclusive about whether Betelgeuse is in the core helium or carbon burning stage of its evolution. Some studies conclude that the star is likely in the late stage of core carbon burning, and a good candidate for the next Galactic Type II supernova. Observations of Betelgeuse's pulsation periods and changes in spectral lines during the star's dimming in 2019 and 2020 indicate material movement and shedding, further supporting the red supergiant stage and its potential for a future supernova. For a 15 solar mass star such as Betelgeuse, the carbon burning phase may be as little as 100 years and so it may already have already have gone supernova and we don't yet know, given that we are seeing the star as it was during the reign of Edward IV and the advent of Caxton's printing press. Some astronomers contend that it is somewhere within its penultimate helium burning stage which for a star the mass of Betelgeuse, could be up to 20 million years in duration. I'd suggest ignoring clickbait You Tube or Tik Tok videos that tell you that the star is imminently about to light up the night sky. Betelgeuse is four times the distance that K2-18b is from Earth so in the case of the latter, we are only peering back in time to the reign of Edward VII and propagation of the first transatlantic radio signal. The red dwarf star that it orbits within the habitable zone, is around 2 billion years old. Perhaps in 5 billion years time when the postulated single celled organisms have evolved into advanced sentient beings that (unlike us?) avoid prematurely destroying their civilisation, instead preserving it, they may gaze at and derive measurements of our own star, by then a red giant that has long since engulfed any traces of our own. Only 6% of presently observable galaxies remain reachable meaning 94% already lie beyond our reach. So, even if we traveled at the speed of light, (which according to relativity is impossible since it would require an infinite amount of energy), currently, we’d never catch up to these galaxies. Each year, another 160 billion stars - equivalent to a major galaxy - become newly unreachable. Meanwhile, the 'unobservable universe' which encompasses all that is beyond the reach of our current technology and understanding. is postulated to be at least 250 times larger than the observable universe, or 7 trillion light-years across. The "observable universe" is defined by the distance light has traveled since the Big Bang, roughly 13.8 billion years ago. This means it's a sphere with a radius of about 46 billion light-years, meaning that we can see objects that emitted light 46 billion light-years ago, nothing further. Since the universe's expansion is demonstrably accelerating, all currently observable objects, outside the local supercluster, will eventually appear to freeze in time, while emitting progressively redder and fainter light. Apropos; objects with the current redshift z from 5 to 10, they will only be visible up to an age of 4–6 billion years. In addition, light emitted by objects currently located beyond a certain comoving distance, (about 19 gigaparsecs), will never reach Earth.
-
As I recall, we played a Europa Conference fixture and the host club, (can't remember whether it was Randers, Rennes or PSV Eindhoven), did their research on our history and unearthed the recording by Jersey Budd which they played pre-match. I may have this wrong...it could have been during the Europa fixtures, but it definitely wasn't Napoli and it was unlikely to have been either Legia Warsaw or Spartak Moscow. Pretty sure it was Rennes or PSV. Anyway, the club quickly adopted it at home.
-
I have a friend in LA who played in a band with him and the grief has hit him particularly hard. Sadly, he is also suffering from what appears to be terminal cancer.
-
Papa V Perpetua? - or have I missed another one? Avoid the 'Ancient Foresters' if you can, full of Headhunters.
-
The question should be, how quickly can you get away from the King Power Stadium?
-
You can see all of this in the Leicestershire countryside. Jackdaws are actually very common across the UK. They tend to nest in small groups unlike the rookeries you'll see. They like to build nests in tree hollows, but in urban areas any cavities will do, and they particularly like chimney stacks, a wall or an attic. They are very, very intelligent like most of their corvid cousins and can recognise you and even respond to a facial expression. Depending on where you are, you will eventually see ravens if you venture up the Northumberland coast (which is wonderful). Puffins, razorbills, guillemots, shags, cormorants, kittiwakes, and terns are frequently seen along the coast. In the Kielder Forest wild boar are present. It's also part of England's Dark Sky park,
-
-
Imagine if the current rumours about the end of the road for the Doctor and the Amazon reboot were actually true - I truly f****g despair. Is nothing sacred or protected? Some of the new era storylines that compromised the history and continuity were bad enough, but a rebrand for a global market would be insufferable. A purple TARDIS for the Tik Tok generation? Reinventing the original story? Harry Styles as the first Doctor. I guess it can't be coincidental that these rumours emerged two days ago. Hilariously this is confirmed by Google's absurd generative AI overview - a feature which they have now been forced to add a disclaimer to.
-
Rode into work today, slightly premature although it'll be a pleasant 18°C by early afternoon. At 6.30am however it was near freezing. Factor in the wind chill on a bike and a 45 minute ride, by the time I arrived it felt like my fingertips had been individually smashed by a ball peen hammer.

-
For the reasons discussed in our comments - and it isn't supposed to be a trustworthy indicator and it isn't a diagnosis. However, it is the best that we have for possible early detection of prostate cancer. And to stress, it is not a diagnostic tool. If it is raised, the next stage would be DRE, then an MRI scan and biopsy. Prostate cancer kills one man every 45 minutes in the UK. Effective early detection is the key to reducing this mortality rate. The PSA test simply measures the level of PSA in your blood and doesn't purport to be anything other than that so forget the notion of false positive or false negative.. It does not specifically test for cancer and should not be regarded as such. A PSA above the typical level for the age range may be a sign of prostate cancer. However, two-thirds of cases of raised via PSA are due to noncancerous conditions such as prostatitis and BPH.
-
-
Agree - particularly in terms of awareness and identification. However, from my consultant's perspective, previous anecdotal diagnosis and treatment by an overseas health system over two decades ago had little bearing upon the evidence based medicine yielded by my MRI and biopsy results. They can only go on the data in front of them. I was told in 2006 that it had never missed a male in the family going back two generations which was a crucial heads up and has great value in terms of cognisance of the disease and recognition of the risk. I was also told that it was a very aggressive form but all indications are that this isn't actually the case and in the absence of an identifiable genetic link, in my case, we can only go with what we know so the supposed family history has little value other than the early warning that I received.
-
This is so crucially important and recommended by Prostate Cancer UK.
-
Yes, good point, and I intended to add that the MRI scan is by no means definitive. In my case, the template biopsy supported the findings. However, as I also mentioned, even then, there may be a proportion that are undersampled or even yield false negative results. Furthermore, going back to my speculation, the MRI does not tell you what the cells are doing within the tumor. So although three years after my diagnosis there appears to be zero growth, it is not known whether the cells are mutating nonetheless. I suspect in my case this has been discovered very early and there is a chance that there is an unidentified genetic mechanism that triggers eventual change meaning that I may well need treatment for a higher grade within the next decade, even though Gleason 6 does not tend to evolve into something worse. It could also be that the overtreatment which afflicted so many historically was exactly what happened two decades ago with my Father. Like I said, given diagnosis, my consultant attached very little significance to the family history or the relevance of the Irish healthcare system two decades ago.
-
Absolutely. It isn't strictly a biomarker and the limitations are clear, such as being organ-specific but not disease-specific which in the past has lead to false positives and overdiagnosis. However it does provide an early warning system for further diagnosis and I would urge anyone with rising PSA or above the national benchmark of 3ng/ml to put pressure on their GP for a DRI or ideally MRI scan. This was lowered from 4ng/ml in the absence of a screening programme. PSA can fluctuate naturally and certain activities can compromise the blood test results such as having sex or vigorous exercise 48 hours before. Key indicators are the velocity and the doubling rate. The size of the prostate gland should also be taken into account - a smaller prostate means that in terms of volume, the PSA figure could be more significant for someone with a prostate the size of a citrus fruit. There are other conditions that can cause PSA to rise rapidly, it doesn't necessarily mean that it is cancer, but it should then prompt investigation. Also be aware that a PSA test does not tend to be included in well man checks any longer. You have to request them. My GP could not find any abrasions either. He concluded that although the prostate was very enlarged he was 99% certain I did not have cancer and begrudgingly referred me for an MRI scan owing to the fact that I stressed that the PSA velocity was high (had risen from 3.3 to 4.3ng/ml in six months), and that there was a family history of the disease. Turned out my prostate isn't enlarged at all, in fact it is under sized (PSA density of 0.18) and that I did have prostate cancer. So the GP diagnosis was 100% incorrect. I was referred for an MRI scan in August 2022. The result was PI-RADS 4 (a high likelihood of clinically significant prostate cancer) T2aN0 (right posteromedial apical peripheral zone) meaning I had suspected stage 2 cancer and that all indications were that it was contained. As result, I was referred for a TRUS biopsy, but due to machine failure, I had the trans perineal template procedure instead, which is more accurate. I then had to wait three and a half months on the diagnostic pathway to find out what grade and how aggressive the cancer was. The NICE guidelines are 28 days - this was 107 days after the MRI result! To provide some context, I tracked down my rogue Irish biological father in Dublin back in 2006. The first thing he told me was that every male in the family had experienced prostate cancer and that it was a very aggressive type (albeit the fact that prostate cancer is slow growing compared to some other forms of the disease). Understandably I was expecting bad news and I was fully prepared for that, but my results consultancy kept getting cancelled. After the sixth time, I jumped in the car with a bundle of letters and drove down to Urology. A very professional and empathetic staff nurse was aghast at the situation and arranged for me to see a doctor immediately. He sat me down and I nearly fell off my chair when they gave the results of the biopsy as Gleason 6 (3+3) (Cambridge Prognostic Group 1 Disease) which is the best possible outcome next to being told you don't have cancer and means that the cells look almost like normal. I can't account for why this has afflicted other males in the family so severely but not me. There are two possibilities. The first is that any cancer causing gene has skipped me and that this is merely coincidence. It is after all one of the most common cancers in the UK. There is no specific gene that we know of that is expressly related to prostate cancer, but many that cause it. Hold that thought. The second is that for the time being I have Gleason 6 cancer, but some unidentified genetic instability may yet cause this to evolve into a higher grade. My initial consultant wasn't in the least bit interested in the family history and certainly saw no relevance in the fact that my Father and Uncle were diagnosed treated in Ireland two decades ago far less, what went on before. He was only interested in the data and the medical evidence before him and the now, which is fair enough. The rest was conjecture. We can only go with what we know. I opted for active surveillance. At this stage there is no point in treating something that doesn't need treating although some with a similar grade have gone straight for brachytherapy or a nerve sparing prostatectomy to purge the cancer from the body. As one particular oncologist reminded me several times, it's not as much physiological but psychological aspect of active surveillance and some understandably don't want to countenance the idea of cancerous cells being in their body no matter how benign. If I elected for either I would almost 100% be cured. Active surveillance is relatively new and we still don't possess much data. However, overtreatment is undeniable and Gleason 6 tends to be something that you die with as opposed to dying of. Also worth adding here however is that 20-30% of biopsies can under sample. So I have my PSA checked twice a year. I no longer have face to face or even telephone consultancies as of this month, which I can only attribute to high clinical load, hence the frequent cancellations when I was on the diagnostic pathway. My PSA is currently 5.5ng/ml and although they are keen to point out the fluctuations along the way, I am also quick to remind them that this is an overall sustained rise. If it continues I will have another biopsy. I have a reasonably high pain threshold, but that was not something that I was particularly eager to experience again. My consultant that performed it who kept hollering "direct hit" and "bang on target" said that with an attitude like that, I'd have him out of a job in months. He liked to refer to it as "death by a thousand cuts". Pretty sure he hadn't detected my gallows sense of humour and it makes you wonder how many complaints have been filed against him in the past. I thought it was quite amusing. I have had two MRI scans since the initial one (the most recent in January of this year), and they all indicate stagnation and zero growth of the lesions which is consistent with Gleason Score 6. However that does not necessarily mean that the cells within are not undergoing change and eventually another biopsy is inevitable and warranted. Apologies for the length of this, but I'd just like to mention two more things. To those that have Prostate Cancer, I would highly recommend contacting the Institute of Cancer Research at the Royal Marsden Hospital. I volunteered for/participated in their 'Precision Medicine in Prostate Cancer' research study. I applied for and was refused genetic counselling by the NHS because my cancer hasn't metastasised, so I wasn't eligible (I thought the general idea of it was to prevent that in the first place). My DNA was sent to a lab in the states (one for the tin foil hat thread), to establish whether I was carrying any cancer related gene and to assist their research into better understanding of the disease. As I said earlier, there is no specific gene expressly related to prostate cancer but there are some very nasty ones that can cause it such as BRCA1 and BRCA2. I wanted to be sure that these were not going to be passed on to my daughter which can also cause ovarian and breast cancers for example. The coding regions of genes were sequenced using an oncogenetics methodology and over 40 were tested for. None were identified although it is important to understand that this is based on our current knowledge and I suspect that there may be an undiscovered genetic link to my cancer. I don't know whether the project is still currently underway but for those in the UK it is certainly worth pursuing depending upon diagnosis. Secondly, I would urge anyone reading this over the age of 40 to regularly check their PSA - and to remember, an elevated figure does not necessarily mean that you have prostate cancer, but it will promote further investigation. This is a stealth killer that tends to be asymptomatic until it escapes. Knowing that it's there beforehand is half the battle won.